
 Biography
Biography Gallery
Gallery Contact
Contact Category
Category
![]() » POLYCYSTIC OVARY SYNDROME (PCOS) » CLINICAL PICTURE OF POLYCYSTIC OVARY SYNDROME
» POLYCYSTIC OVARY SYNDROME (PCOS) » CLINICAL PICTURE OF POLYCYSTIC OVARY SYNDROME
CLINICAL PICTURE OF POLYCYSTIC OVARY SYNDROME
 01.03.2019 19:19
Author: Asst. Nebojša Zečević, MD, PhD
01.03.2019 19:19
Author: Asst. Nebojša Zečević, MD, PhD
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in women in reproductive age and the main cause of female infertility.

Excessive body hair, irregular periods, infertility, obesity and hormonal disorders may be symptoms of polycystic ovarian syndrome (PCOS). An ultrasound examination is the starting point for accurate diagnosis, after which a definitive diagnosis is given.
Polycystic ovary syndrome can affect fertile women, with or without excessive body hair, infertile women with a regular menstrual cycle, and even women with abnormal bleeding from the uterus (metrorrhagia). In contrast, excessive body hair, irregular menstrual periods (oligomenorrhoea) and infertility can also be found in women without enlarged ovaries.
Regardless of whether the ovaries are enlarged,Polycystic ovary syndrome shows:
the presence of numerous small cysts (subcortical follicles) most often size - 2 to 6 mm,
enlargement of the central stroma (the centre of the ovary),
thickened capsule.
This is also known ashyperandrogenic ovarybecause the synthesis of male sex hormones (androgens) isexcessively increased.
PCOS signs:
1. The average age of occurrence of the first menstrual period (menarche) is about 12.3 years.
2. Menstrual disordersoccur in the majority of cases and occur immediately after the first period.
3. Excessive body hair (hirsutism) is noticed immediately before or during the time of the menarche,
4. Most patients were obese before the first period.

These women patients often complain of oily skin, hair and acne on the face, on the back and the shoulders. There can be somethinning of the hairon the top of the head or so called temporal balding.
HIRSUTISM (EXCESSIVE BODY HAIR )
This symptom is most badly experienced by women and is often the reason for the first visit to the doctor. Ultimately, it is a sign of an elevated level of androgens - male sex hormones (hyperandrogenism). However, the level of androgens in the blood is not always directly related to the degree of hirsutism.
Excessive body hair is not always present in PCOS: some patients do not have it, some patients experience it in a mild form andvery rarely in a very high degree with signs of the development of male secondary sexual characteristics.
Excessive body hair in women (hirsutism) is most common in women in the so-called androgen sensitive areas, where body hair is expected in men - between the nose and upper lip,cheeks, beard, around nipples, along the central abdomen line and under the navel and upper third of thighs inwards. In these patients, the occurrence of androgenic alopecia (baldness) is rare.

Excessive body hair is a common symptom of PCOS
MENSTRUAL DISORDERS
Irregular menstrual periods(oligomenorrhoea) is a very common condition and occurs in about 75% of cases. About 25% of women with amenorrhea (complete absence of menstrual periods) have PCOS. However, according to various studies, 8-25% of women with PCOS have regular menstrual cycles.
INFERTILITY
It occurs in about 74% of women with PCOS as a result of a chronic absence of ovulation (anovulation) or a reduced number of ovulatory cycles. However, almost 1/4 of women with PCOS get spontaneously pregnant, i.ewithout prior medical treatment.
OBESITY
To a lesser or greater degree, obesity is present in more than 50% of women with PCOS. The development of menstrual irregularities is closely related to the degree of obesity, while weight loss usually leads to regular menstrual cycles.
HORMONE LEVELS
- Elevated LH (luteinizing hormone),
- Increased LH response to GNRH
- Normal or reduced FSH, ratio LH / FSH greater than 1.5
- Normal or elevated levels of testosterone
- Normal or elevated androstenedione
- Elevated or normal DHEA-S level
- Low SHBG (sex hormone binding globulin)
- Elevated estrogen / estradiol ratio
- Elevated insulin levels (before or during sugar intake)
All of these changes in the hormonal status of PCOS, and above all the elevated LH / FSH ratio, lead to a disruption in follicular maturation, increased production of male sex hormones, suspension of growth and follicular maturation, as well as absence of ovulation.
In about 10-30% cases with this syndrome there is an increase in the level of prolactin (hyperprolactinaemia), but as a rule, it is mild.
DIAGNOSIS
Ultrasound examination is not only the most important for the diagnosis of polycystic ovarian syndrome, but also crucial for some therapeutic procedures, primarily the induction of ovulation. Patients can have transvaginal ortransabdominal (for virgins) ultrasound examinations.
The ultrasound usually detects an enlarged or normal ovary with the presence of a number of follicles / cysts (4-6 mm), most often peripherally placed beneath the superficial ovary capsule and centrally located ovary center (hyperechoic stroma). This appearance of the ovary is typical for the condition. Thus, along with someother parameters, the diagnosis is easily made.
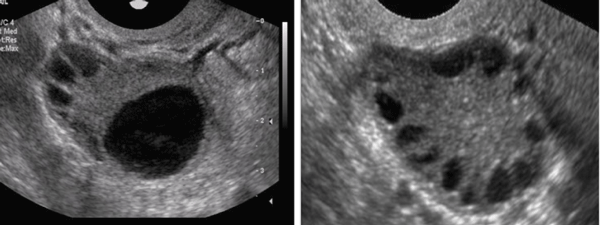
Ultrasound images: normal ovary and polycystic ovary
After the ultrasound examination, according to the protocol, it is necessary to carry out the following analyses:
Day 1: MC: FSH, LH, SHBG, testosterone, androstenedion, prolactin profile (8, 11 and 13h), TSH, DHEA - S
2. 21 days MC only progesterone from the blood
3. Vitamin D from the blood.
4. OGTT with 75 g glucose 0, 30, 60, 90 and 120 minutes with insulins 0, 60 and 120 min.
INSULIN RESISTANCE - IR
IR is at the very root of PCOS. Insulin is a hormone secreted by islet cells within the pancreas,in response to blood sugar (glucose) levels. After a meal, there is always an increase in blood glucose, and therefore insulin. Their values fall after a certain amount of time. Carbohydrates and food proteins boostinsulin. The role of insulin is to transport glucose and amino acids to the cells of the whole organism, while the amino acids go into the muscles.
The excess of calories burned is stored in the form of fat deposits.
When the blood sugar level is chronically elevated (due to improper diet, stress, other disorders), the level of insulin is constantly high and over time the cells lose the ability to respond adequately, i.e become resistant to insulin. The insulin is then intensified. Consequently, the pancreas is exhausted and it eventually loses the ability to produce this very important hormone. This leads to the development of diabetes.
In PCOS, elevated insulin (also in the case of insulin resistance) stimulates the growth and reproduction of ovarian cells surrounding the egg cells, which leads to increased production of male (testosterone) and female (estrogen) hormones. Healthy ovaries produce smaller amounts of male sex hormones (androgens), but convert it into estrogen (female hormone). In the case of IR, enhanced production of androgen exceeds the capacity of the ovaries and therefore there is excess of androgen. Eventually, all this leads to disorders of ovulation, oily skin, hair, excessive body hair, acne ...
Often patients feel reactive hypoglycaemia, or sudden drop in sugar when they have to take something sweet.
Diabetes (type 2) in close relatives of these patients is quite common, especially after the age of 50.
Why is a glucose test needed
OGTT (oral glucose tolerance test ) is the main diagnostic test that patients with PCOS have to do. The result of this test may indicate a disorder of sugar regulation, i.e insulin resistance. It is performed mostly with 75 grams of sugar taken by the patientbefore any meal. After thata blood sample is taken and glucose measured at 0, 30, 60, 90 and 120 minutes, with insulin measurements at 0, 60 and 120 minutes. Then, by calculating the Homa Index, the presence of insulin resistance is determined.
VITAMIN D IS VITAL
Vitamin D concentration in healthy women is on average higher than in women with PCOS. Numerous recent studies suggest that vitamin D supplementation reduces insulin resistance and stimulates AMH (Anti-Muller hormone) which is an indicator of ovarian reserve with egg cells. The vitamin D deficiency also reduces the success of the process of fertilization (IVF). The determination of Vitamin D level and supplements (if necessary) are advised to women preparing for IVF.
TREATMENT OF PCOS
The treatment depends on all the needs of the patient and her reproductive status (pregnancy plan).
Irregular menstrual cyclesaretreatedwith contraceptive pill combinations (estrogen and progesterone) or with gestagenic preparations (synthetic progesterone).
Excessive body hair is treated with contraceptive drugs, medicines with antiandrogen (for the control of male hormones) or with anti-angiogenic agents.
Infertility is treated with medicines for stimulation of ovulation, drugs for reduction of IR, vitamin D, and sometimes with surgery (ovarian driling). The stimulation of polycyctic ovaries should be performed with special care so the patient does not develop hyperstimulation syndrome. The drug dosagein the case ofpolycystic ovarian stimulation must be accurately determined.
Tags: polycystic ovary syndrome, insulin resistance,infertility, excessive body hair, hirsuitism, PCOS, ovarian drilling
Tags: polycystic ovary syndrome insulin resistance infertility excessive body hair hirsuitism PCOS ovarian drilling






© 2018 by nebojsazecevic.com | All right reserved
Design by draganmarkovic.net
Use of cookies. This site uses cookies to analyze traffic and improve the user experience. By continuing to use the site you represent that you agree to the use of cookies.
OK