
 Biography
Biography Gallery
Gallery Contact
Contact Category
Category
![]() » GENETIC DISORDERS AND THE FETUS » MOLECULAR KARYOTYPE, THE MOST COMPLETE PRENATAL GENETIC TESTING
» GENETIC DISORDERS AND THE FETUS » MOLECULAR KARYOTYPE, THE MOST COMPLETE PRENATAL GENETIC TESTING
MOLECULAR KARYOTYPE, THE MOST COMPLETE PRENATAL GENETIC TESTING
 24.10.2018 17:08
Author: Asst. Nebojša Zečević, MD, PhD
24.10.2018 17:08
Author: Asst. Nebojša Zečević, MD, PhD
Molecular karyotype (CGH array) is a new method in prenatal genetic testing, which can detect genetic malformations in the fetus that would not otherwise be detected before childbirth

For years, doctors (and future parents) have believed that if a pregnant woman performs a classical amniocentesis, which only sees numerical aberrations (a full extra chromosome or the entire chromosome is missing) and the result is even, the child will be healthy. Practice has shown that it is not always the case. Data show that, for example, 15% of children with delayed development, congenital disorders or some form of autism have a normal conventional karyotype.

A conventional karyotyping, which has been routinely done for 30 years, includes procedures that chromosomes color, agree and only quickly look through the microscope: whether they are all there or have major defects. What is often missed are deletions (situations in which a small parts of chromosomes are missing) and duplications (when there is a surplus of chromosomes) that are less than 10 Mb (microproplications and microdellations). The microscope "does not see" these small mistakes with conventional karyotyping. They can only be seen through a CGH array (Comparative genomic hybridisation) or molecular karyotype.
Both the old and the new methods have some common characteristics: in both cases, the material obtained by amniocentesis or chorionic villus sampling (CVS) is analyzed. Both methods show changes in the total number of chromosomes and major irregularities.

Prenatal diagnosis can be performed by conventional cytogenetics and molecular genetics.

With conventional methods low resolution microscopes do not reveal the tiniest errors.
What makes a difference is the fact that molecular karyotype (CGH array), in addition to any change in the total number of chromosomes and major irregularities (detected by conventional karyotype), can also reveal 512 different microdeletions and microduplications (extremely small genetic anomalies) that can predict a serious clinical picture, sometimes much more severe than that of Down syndrome. For example, DiGeorge syndrome, TAR syndrome, Angelman, Prader-Willi syndromes and many other microdeletions and microduplications that are not described as specific syndromes - it is established which genes are at the place where the problem is and then by using the on-line base (ONIM) we can see how it affects children.
An additional advantage of the application of molecular karyotype in prenatal diagnosis is a shorter time until the complete finding is issued - normally only 5 to 7 days.
The test can be performed from 14 weeks of gestation.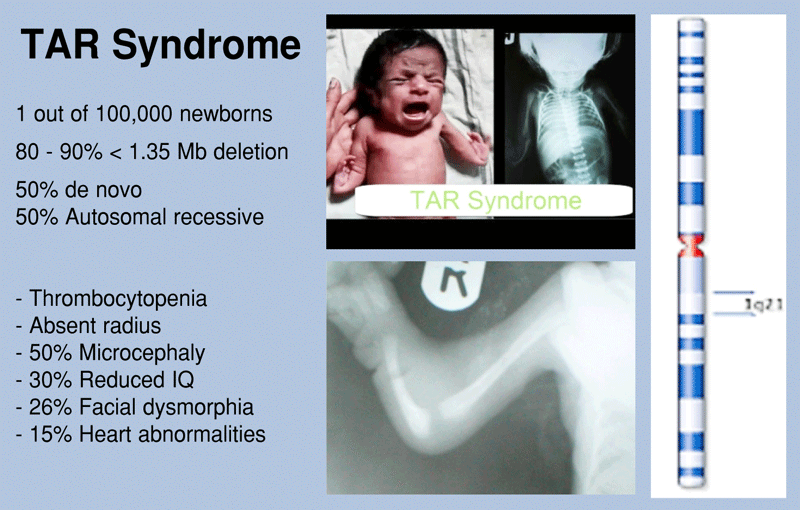
TAR syndrome

DiGeorge syndrome
Who is molecular karyotype for?
In some developed countries, the standard is that after amniocentesis, the amniotic fluid sample is always sent for the most complete analysis, or molecular karyotype.
In our country, this analysis is done if a gynecologist suspects that the irregularities on chromosomes are extremely small, that is, they cannot be detected by the usual methods.
Molecular karyotype is recommended for all pregnant women who have decided on amniocentesis and those who want to obtain a more complete analysis than can be obtained through a conventional karyotyping.
In families where there are genetic abnormalities that are not confirmed by the usual tests, amniocentesis and analysis of molecular karyotype are advised.
Tags: Genetic testing Malformations in the fetus Molecular karyotype CGH array TAR Syndrome DiGeorge Syndrome






© 2018 by nebojsazecevic.com | All right reserved
Design by draganmarkovic.net
Use of cookies. This site uses cookies to analyze traffic and improve the user experience. By continuing to use the site you represent that you agree to the use of cookies.
OK